There have been lots of buzz regarding artists taking plastic surgery to get their beauty enhanced. In the case of artists taking plastic surgery, there are lots of public perceptions about why they would have undergone the knife work. Of the most forefront reason is that they consider some parts of their body as their most hated enemy. Lots of artists have surgery on their nose, breast, and butt. The other thing which is related to taking the surgery is the desire to keep their fabulous look intact. It is without a doubt clear that most artist would be tempted to stay at the top of their career. This can be realized through knife work. One of many artists that have been speculated to have undergone the knife work is Kim Novak. Kim Novak was born on February 13, 1933, in Chicago. She is best known as an American actress, model, and television reality host. She started her career in 1954 just at the age of 21. She then burst her popularity with her leading role in the film Picnic in 1955. The other films that she has starred include The Eddy Duchin Story, The Man with the Golden Arm, Pal Joey, Jeanne Eagles, Alfred Hitchcock, and Middle of the Night. Kim Novak is best known as one of the most sparkling female actresses in her generation. However, her beauty has been deteriorated by the disastrous Kim Novak plastic surgery.

Source: isuwft.com
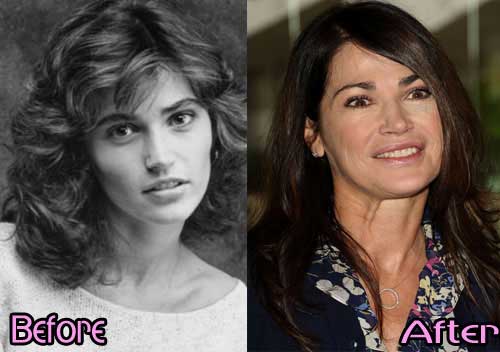
Another case of plastic surgery disaster?
No one would deny her beauty and bright look at that time. With the fame she had at that time, some people started to forage for the bad sides of Kim, one of which is her plastic surgery rumors. Kim Novak came as a total shock when she got old. The rumors have taken the issues even higher since there have been lots of photo on the internet which are meant to pose the differences she has before and after the plastic surgery. After years of speculation, the rumors about her surgery which has turned disastrous. As what happened to the most artist, there have been lots of plastic surgeries that end up happy. However, some others have gone wrong and lead to the disastrous outcome. The rumors about Kim Novak are deemed as one of an awful plastic surgery of all time. As you can see in the newer photo, there seems to be no remain of the old time beauty she had. Her face has turned into the monstrous face which most people would be afraid of. You will see that there is a frightening line on her face, which appears as forced a smile. Also, there are lots of wrinkles around the smile. People assumed that the disastrous look is due to the excessive use of botox injections she had in the past.

Kim Novak Cosmetic Surgery Failure – What else have been disastrous?
Well, perhaps, Kim Novak plastic surgery can be a warning for those who consider having plastic surgery to escalate their beauty. There are of course lots of things which should be pondered before undergoing plastic surgery. In the case of her plastic surgery, there is a salient sign of plastic surgery has come as a failure in her face. Instead of looking gorgeous and sparkling as most people desire, Kim Novak has turned into a cosmetic monster through the surgery. The deficiency of her plastic surgery has been attributed to some excessive use of botox injections or fat fillers. Most surgeons have claimed that the excessive use of those fillers can be awful in that they may create the unnatural and awful look.